Overview
The novel coronavirus (COVID-19, severe acute respiratory syndrome coronavirus 2; SARS CoV-2) pandemic has highlighted and exacerbated many racial health inequities that existed well before this public health crisis. People of color are disproportionately contracting COVID-19, and because they are more likely to have underlying health conditions, are also facing an increased risk of severe illness and mortality from COVID-19 (CDC, 2020). While COVID-19 has pushed racial health inequities into the national spotlight, the underlying differences in social, economic and environmental conditions that have given rise to inequities in COVID-19 infection, transmission and severe illness are not new (CDC, 2020).
Race- and place-based discrimination, both past and present, have created and actively maintained racial residential segregation. Racial residential segregation has systematically shaped characteristics of the built environment that may increase susceptibility to not only COVID-19, but other underlying health conditions that increase the susceptibility to and severity of illness from COVID-19. Racial residential segregation may impact health through poor housing conditions, disparity in educational and employment opportunities, inadequate transportation infrastructure, access to healthcare and economic instability (Barber et al., 2020; Bailey et al., 2017; Diez Roux and Mair, 2010). Where people live impacts their exposure to health promoting resources and opportunities (i.e., access to quality food, recreation, healthcare, etc.) as well as exposure to health damaging threats (i.e., environmental pollutants, poor housing quality, etc.) (Diez Roux and Mair, 2010). Robust literature has documented racial residential segregation as a determinant of racial health inequities (Williams & Collins, 2001; Williams, Lawrence, & Davis, 2019; Bailey et a., 2017; Kramer & Hogue, 2009; Gee & Ford, 2011; White & Borrell, 2011). Racial residential segregation has been linked to cardiovascular disease (Kershaw et al., 2015), hypertension (Kershaw et al., 2011; Barber et al., 2018), diabetes (Barber et al., 2018), obesity (Pool et al., 2018), asthma (Alexander & Currie, 2017) and many other adverse health conditions (Beyer et al., 2016; Morello-Frosch & Jesdale, 2006; Debbink & Bader, 2011; Mehra, Boyd, & Ickovics, 2017; McFarland & Smith, 2011). Structural racism and racial residential segregation are associated with stark differences in neighborhood resource distribution, concentrated disadvantage and health. These obstacles are not recent in origin, but are rooted in historical policies and practices.
Epidemiology of SARS COV-2
SARS-CoV-2 is a novel coronavirus belonging to the β-coronavirus cluster (Sun et al., 2020). The first cases of SARS-CoV-2 were documented in December 2019 in Wuhan, China (Jayaweera et al., 2020). The outbreak was declared a pandemic by the World Health Organization (WHO) on March 11, 2020. The most common symptoms of SARS-CoV-2 include fever, cough, fatigue, muscle pain and dyspnea.[13] SARS-CoV-2 is transmitted by contact with respiratory droplets either person-to-person or person-to-environment, and, in clinical and indoor settings, aerosol (airborne) transmission has been documented (Jayaweera et al., 2020). Standard epidemiologic parameter estimates, including transmission rate and case fatality rate, vary by country and study due to differing population structures, testing coverage and reporting.
In the U.S., minorities, particularly Black and Hispanic individuals, are disproportionately infected by SARS-CoV-2. National data from the Centers for Disease Control and Prevention (CDC) through May 28, 2020, detail that Black and Hispanic residents are three times more likely to be infected and two times as likely to die from COVID-19 compared to Whites.[14] These disparities have been ascribed to differential access to health care, household size and essential worker status, however, the root cause of these inequalities is structural racism.[15]
COVID-19 health risk factors
Information about COVID-19 is evolving as scientific experts learn more about this disease. At the time of this report, the latest revision from the CDC on June 25, 2020, reported that people of any age with the following underlying health conditions have an increased risk for severe illness from COVID-19: chronic kidney disease, COPD (chronic obstructive pulmonary disease), obesity, severe heart conditions, type 2 diabetes, sickle cell disease and those with a weakened immune system from solid organ transplant (CDC, 2020). Additionally, the CDC reports that people with the following conditions might have an increased risk for severe illness from COVID-19: asthma, hypertension or high blood pressure, type 1 diabetes, cerebrovascular disease, cystic fibrosis, neurologic conditions, liver disease, those who are pregnant, pulmonary fibrosis, those who smoke, thalassemia, and those with a weakened immune system from blood or bone marrow transplant, immune deficiencies, HIV and use of corticosteroids or other immune weakening medicines (CDC, 2020).
HOLC residential security maps & public health
While measures of racial residential segregation are commonly used as a proxy for structural racism, to date, there have been few studies which empirically measure the effect of structural racism on health (Bailey et al., 2017; Krieger, 2014; Hardeman et al., 2018). However, after the recent digitization of the HOLC residential security maps, several studies have evaluated HOLC grades, as a measure of structural racism, in relation to current health outcomes and social determinants of health (Huggins, 2017; Jacoby et al. 2018; McClure et al. 2019; Namin et al., 2020; Transgenstein et al., 2020; Hoffman et al., 2020; Nardone et al., 2020; Krieger et al., 2020; Krieger et al., 2020). Hoffman, Shandas and Pendleton (2020) and Namin et al. (2020) examined cities across the country, while the remaining studies evaluated HOLC grades within single cities (Huggins, 2017; Jacoby et al. 2018; McClure et al. 2019; Transgenstein et al., 2020; Krieger et al., 2020) or cities within a state (Nardone et al., 2020). While predominantly using ecological models to evaluate neighborhood level health outcomes, a few studies have utilized multilevel models to inform individual level inferences (McClure et al., 2020; Krieger et al., 2020; Krieger et al., 2020). From examining environmental exposures (Hoffman et al., 2020; Namin et al., 2020), preterm birth (Krieger et al., 2020), cancer state at diagnosis (Krieger et al., 2020), crime (Jacoby et al. 2018), asthma outcomes (Nardone et al., 2020), alcohol outlet clusters (Transgenstein et al., 2020) and self-reported health (McClure et al. 2019), these studies have collectively raised awareness on the legacy of government-sponsored redlining practices that were initiated in the 1930s on current population health.
Racism, segregation & COVID-19
Further, amidst the COVID-19 pandemic’s disproportionate impact on the country’s Black population, Barber et al. (2020) examined racial residential segregation and COVID-19 cases in Philadelphia, guided by theoretical frameworks for studying structural racism. The HOLC’s historical practices of redlining and other discriminatory lending practices were instrumental in driving the stark segregation seen in Philadelphia today. While not explicitly measuring HOLC redlining maps, Barber et al. (2020) acknowledge how these historical processes established the physical, economic and social conditions that are giving rise to racial inequities in COVID-19. They illustrate how structural racism embedded in our interlocking social, legal, economic and political systems interact to drive disproportionate prevalence of COVID-19 infection, transmission and mortality in Black communities (Barber et al., 2020). Their results showed that the most segregated neighborhoods in Philadelphia were more likely to have structural susceptibility to COVID-19 (a measure encompassing neighborhood indicators that increase the likelihood of exposure and community transmission, limit ability to access testing and treatment, and capture economic hardship). Further, the COVID-19 case rate in the five most segregated neighborhoods was twice that of the COVID-19 case rate in the five least segregated neighborhoods. These findings suggest that segregation acts as a structural driver of racial inequities in Philadelphia and calls for both short- and long-term solutions that center structural racism and health equity in the COVID-19 response.
Public health indicators
Life expectancy at birth is a common indicator of population health and social development, representing the average number of years a newborn is expected to live under current age-specific mortality rates (WHO, 2014). Life expectancy accounts for mortality risks and trends, thus is used to track improvements in health (WHO, 2014). While overall life expectancy has steadily risen since 1900 in the United States, racial inequalities in life expectancy, particularly between Blacks and Whites, have persisted (Kochanek, Arias and Anderson, 2015; Harper et al., 2007). Studies at both an individual and neighborhood level have found that exposure to racial residential segregation was associated with shorter life expectancy among Blacks (LaVesit, 2003; Collins and Williams, 1999). Additionally, among the 500 largest cities in the United States, the difference in life expectancy ranged between 20 and 30 years depending on which neighborhood an individual lived in; this gap was largest in cities with stark racial residential segregation (NYU NewHub, 2019).
Mental health is increasingly monitored as an indicator of population health and chronic disease burden (CDC, 2009). Poor mental health can adversely impact social engagement, functioning, health behaviors and physical health (CDC, 2015). People of color bear a disproportionate burden of unmet mental health needs (Office of Surgeon General, 2001) and racial residential segregation differentially shapes access to mental health services (Dinwiddie et al., 2013).
Gaps in our hypothesis
Previous work by NCRC identified HOLC “Hazardous” graded neighborhoods as economically disadvantaged, with much higher proportions of low- and moderate-income (LMI) families (74%) and people of color (64%) than the higher graded “Best” neighborhoods. The present study explored the legacy of HOLC residential security maps, as a measure of structural racism, on current health indicators that are considered risk factors for COVID-19 infection and severe illness, making it one of the first inquiries into historical redlining in cities across the nation on numerous present-day neighborhood health outcomes.
How might redlining from 80 years ago influence current health? A recent paper by Krieger et al. (2020) outlines specific pathways which provide a theoretical linkage for the association of redlining and segregation, neighborhood disinvestment and health. This pathway model is modified in Figure 1 to show the historical development and linkages between residential segregation and health outcomes. Public policies, instituted beginning in the 1890’s and 1900’s and extending through passage of the Fair Housing Act in 1968, provided the institutional and legal structure of segregation. These included local codification of segregation in residential areas, racially restrictive covenants and deeds and, in some cases, regulations on land-use (Rothstein, 2017). Governmental policies and social structures of the time buttressed residential segregation, with mortgage and insurance redlining establishing neighborhood trajectories of investment and disinvestment. During the post-war period, major changes to the U.S. urban system were underway with suburbanization, construction of the national highway system and “block-busting” and “White-flight” from central cities (Jackson, 1985). This migration and reconfiguration of urban and suburban areas shaped patterns of consumption and impacted availability for a wide range of neighborhood services from food availability to financial services, healthcare (Cohen, 2003) and exposure to disamenities and environmental hazards (Pulido, 2000). The differential availability of educational and employment opportunity, services and exposure to hazards impacts the physical and mental wellbeing of people living in segregated neighborhoods (Dreier et al, 2004).

This study expanded on prior work in order to examine the association of the HOLC residential security grades with adverse neighborhood health and other forms of disadvantage. The HOLC low-graded areas of cities are historically disadvantaged neighborhoods where the combination of segregation and disinvestment created the circumstances of concentrated disadvantage for residents, which may operate through numerous mechanisms identified by Krieger et al. to influence current population health. This study assessed statistical associations of the HOLC grading and a range of current indicators of COVID-19 vulnerability.
Design
This ecological study was structured to examine the spatial coincidence of HOLC neighborhood grading and the prevalence of adverse health outcomes and public health outcomes. Two modes of analysis are undertaken: Analysis of Variance (ANOVA) to assess statistical significance of differences in neighborhoods scored by the extent of redlining, and regression equations for effect estimation. The neighborhood HOLC grade was assessed through a “historical redlining score.” The historical redlining score was calculated and divided into quartiles nationally. Regression models utilized health outcome data and data on social and demographic factors as the dependent variable, with the continuous historical redlining score as the primary predictor variable. Additional covariates, including the percent minority population and median age, were used to control for potential confounding of the relationship between the historical disinvestment score and the health and social disadvantage variables.
Study area and data
Data from the residential security maps created by the HOLC’s City Survey program is hosted by the University of Richmond Digital Scholarship Lab as part of their “Mapping Inequality: Redlining in New Deal America” project.[16] The data includes scans of the original residential security maps, along with examiner grading sheets and digitized shapefiles of the neighborhoods. The shapefiles are georectified and suitable for projection and use in geographic information systems (GIS). This archive is an extensive and expanding repository of the maps for cities throughout the United States, and served as our primary source material. census tract level data from the 2019 release of the CDC’s “500 Cities: Local data for better health,” which included small-area estimates from 2016 and 2017, was used as a primary source for most of the health-outcome related variables.[17] Other data utilized included the CDC’s “small-area life expectancy estimates project” for 2010-2015 and U.S. Census American Community Survey five-year (ACS 5-year) data estimates for 2013-2017.[18] [19] [20]
Variables:
Historical redlining score
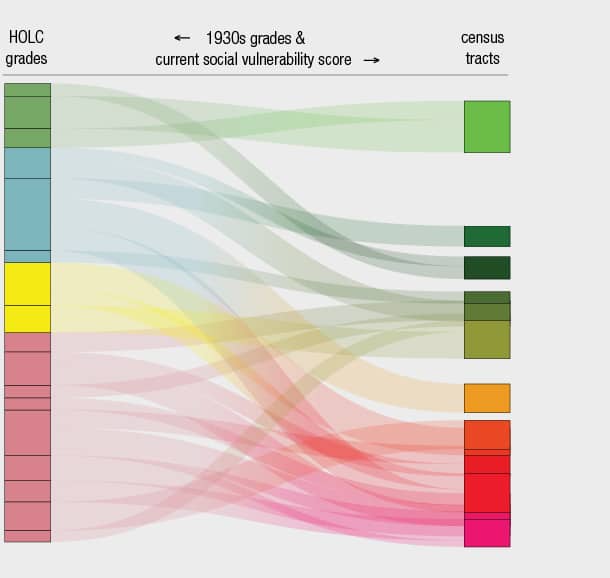
Neighborhoods in the original HOLC maps were based on boundaries established by the HOLC examiners themselves. These do not align with U.S. census tract boundaries, which are adjusted decadallyand can fluctuate considerably as population shifts over time. This spatial mismatch proves a challenge when attempting to analyze present conditions in the HOLC designated areas. To solve this problem, a weighting method was developed in order to establish a historical redlining score as a continuous variable (Figure 2).[21] First, we established the total area of land within each census tract that was graded by the HOLC. Census tracts, in which less than 20% of the land area was graded, were discarded from the analysis as being insufficiently impacted. A total of 12,834 census tracts were classified representing 142 core-based statistical areas (CBSAs) across the country. Next, the total percent of the area within each census tract graded “A=Best,” “B=Still Desirable,” “C=Definitely Declining” and “D=Hazardous” were defined and this percent was multiplied by number values — 1-4 representing each HOLC grade. For example, if 50% of the census tract’s graded area was classified “A” and 50% was “B,” the calculation would be ((1 * 0.50) + (0.50 * 2)) = 1.50. Lower historical redlining scores indicate higher grades, while higher scores up to 4.0 represent a greater portion of the area being scored hazardous and consequently having been redlined.

For the national-level analysis, the historic redlining scores were ranked and sorted into quartiles for comparison purposes. The first quartile represents areas with the least redlining and the fourth represents the highest scores indicative of greater redlining (Table 1). The HOLC maps categorized many more neighborhoods with a low, or “hazardous” grade, than with the highest, or “best” grade. Consequently, the mean of the fourth quartile is 3.94, with a “D” grade being 4.00, while the mean of the first quartile of 1.87 is closer to the numeric value of a “B” grade at 2.00.

Variables relating to demography, socioeconomic status, social vulnerability and specific health outcomes at the census tract level were used in this analysis. Population counts were taken from the U.S. Decennial Census data for 2010. The most recent Census American Community Survey (ACS) 2014-2018 provided five-year estimates for tract level data on the percent of minority residents, median age and percent of the population aged 65 and over. These estimates provided an indication of the prevalence of more vulnerable minority and older populations. The ACS 2014-2018 data also contained variables for the percent of the population that was insured and levels of poverty, indicative of the financial means to access health care and economic vulnerability. For the population health indicators, data from the 2019 CDC “500 Cities” dataset was used, which covered data collected in 2016 and 2017, and aligned well with the census demographic data. Using the CDC 500 Cities dataset, we focused on the prevalence of the following risk factors of increased severity of COVID-19 illness among adults 18 years of age or older:[22] diabetes, hypertension, high cholesterol,[23] chronic kidney disease, COPD, stroke, obesity and asthma.[24] Data on life expectancy at birth obtained from the U.S. Small-area Live Expectancy Estimates Project (USALEEP) was utilized as an indicator of general population health.[25] The CDC also calculates an index of social vulnerability (SVI) to evaluate the resilience of neighborhoods to a wide range of hazards including human and natural disasters and outbreak of diseases, such as COVID-19.[26] Social vulnerability indices are widely utilized in the hazards and public health fields, providing a general indication of community susceptibility or resiliency to a wide range of natural and human-caused disasters. Social vulnerability indices are constructed from a composite of different variables taken from census data that are related to increased community vulnerability.[27]
Statistical analyses
Means and standard deviations for current sociodemographic and COVID-19 health risk factors of census tracts were calculated nationally for all census tracts and then by historic redlining score quartile. Descriptive differences in patterns of disadvantage and COVID-19 health risk factors were formally tested with a One-Way Analysis of Variance (ANOVA), a procedure which estimates the variation between groups of the same variable (Field, 2013). Several conditions for the data in the dataset need to be met for the statistical models classified as ANOVAs to be valid. The data should have equivalent sample sizes, be normally distributed, randomized, with homogeneity of the variance of the residuals. When tests for these assumptions were run, the variables in the datasets had violations of the tests for homogeneity of the variances. Additionally, the sample sizes for each quartile ranged from 1,671 to 3,411, violating the precondition for equivalence. Consequently, more robust tests such as Welch’s test for the equality of the means needed to be employed to successfully assess the overall differences between the groups. Welch’s test indicates whether the overall trend in the difference of means for the first, second, third and fourth quartiles are statistically significant. A Games-Howell post-hoc test was then conducted to evaluate a pairwise comparison of the means for each quartile. The Games-Howell test can be used when sample sizes are different and provides more rigorous confidence intervals than other post-hoc tests. Finally, a series of linear regression models were generated to estimate the association between historic redlining score and COVID-19 health risk factors adjusting for several factors. The first model is unadjusted, the second model adjusts for median age and state where the census tract is located and the third model additionally adjusts for percent of the population within a tract classified as non-White.
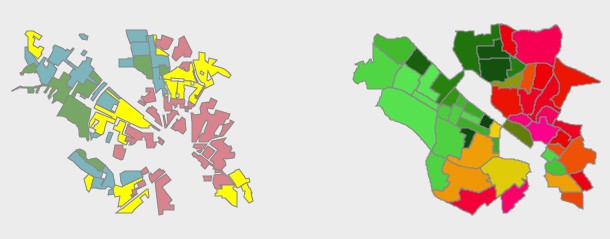
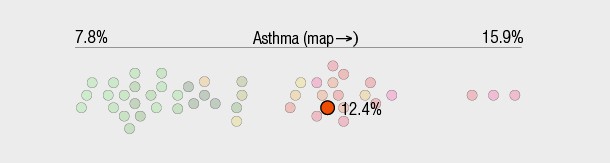
A total of 12,833 census tracts were assigned a historic redlining score. Tract-level sociodemographic characteristics, including the percent minority population, median age and percent poverty were available for 12,833 tracts. For percent age 65 years and older, data was available for 12,829 tracts. Data on estimated life expectancy at birth was available for 11,890 tracts, and for social vulnerability as measured by the CDC’s SVI, 12,830 tracts. Figure 3 provides a map overlay example focused on St. Louis demonstrating the original 1937 HOLC grading, the historic redlining scores with life expectancy and social vulnerability by CBSA quartiles.[28] For all COVID-19 health risk factors, data were available for 10,248 tracts. Table 2 shows the distribution of sociodemographic characteristics and COVID-19 health risk factor prevalence at the national level and by quartile of historic redlining score. On average, census tracts included in this analysis were approximately 46.6% minority populations, had 21.7% living in poverty and a median age of 36.3 years with 13.1% 65 years or older. The mean tract-level prevalence of COVID-19 risk factors were as follows: 31.9% for hypertension, 32.0% for obesity, 11.9% for diabetes and 10.3% for asthma. Average prevalence for COPD was 6.8%, 3.3% for kidney disease and 3.6% for stroke. In addition, the average tract level prevalence for percent of the population with mental health issues was 14.8%.

The distribution of sociodemographic characteristics and COVID-19 health risk factors were then examined by quartile of historic redlining score (Table 2). Quartile 1 included tracts with the lowest levels of historic redlining while Quartile 4 included tracts with the highest levels of historic redlining. A pattern of current disadvantage and higher prevalence of COVID-19 health risks was observed with greater levels of historic redlining. For example, the average poverty percentage increased from 14.3% in tracts in the lowest quartile of historic redlining score to 28.1% in tracts in the highest quartile of historic redlining score. A similar trend was observed with the social vulnerability index. Tracts with higher historic redlining scores had higher average proportions of minority residents (57.0%) than tracts with lower historic redlining scores (34.6%). While the average life expectancy fell from 79.4 years in the lowest quartile to 75.8 years in the highest, differences in the average median age (38.8 years versus 34.4 years) and the average percent of the population aged 65 and older (14.4% versus 11.7%) were higher in the lowest quartile, suggesting that life expectancy declines were not driven by population age distributions.
COVID-19 health risk factors were also patterned by levels of historic redlining score, with higher average prevalence of asthma, COPD, diabetes, hypertension, kidney disease and stroke observed in tracts with greater historic redlining scores. This is despite quartile 1 tracts (i.e., low historic redlining) having higher average median age and higher percentages of people age 65 years and older. The average prevalence of poor mental health also increased from 12.7% to 16.1% in low historic redlining areas compared to high historic redlining areas.

Results of the One-Way ANOVA Games-Howell post-hoc test for difference in the means of the first and fourth quartiles are presented in Table 3. The table shows the difference of the means for each variable contrasting the highest (fourth) and lowest (first) quartiles of historic redlining score. The mean values for percent minority, percent poverty and SVI were all statistically significantly higher in tracts with the highest historic redlining score compared to tracts with the lowest historic redlining score. As expected, average median age, percent of population age 65 years and older and life expectancy are all statistically significantly lower in tracts with the highest historic redlining score. Full results of mean contrasts between all quartiles by sociodemographic characteristics and COVID-19 health risk factors are available in the Appendix.

Table 3 – Results of ANOVA with Games-Howell post-hoc test for significance of the differences – Health indicators with historic disinvestment score divided by quartile nationally. Quartiles 4 and 1 differences only.
Table 4 shows the results from a series of linear models that assessed the association between historic redlining score and average prevalence of COVID-19 health risk factors and sociodemographic variables. A higher historic redlining score was statistically significantly associated with increased prevalence for all COVID-19 health risk factors considered. For example, a one unit increase in historic redlining score was associated with a 1.64% increase (95% CI: 1.52, 1.76) in tract average prevalence of diabetes. All associations between the historic redlining score and COVID-19 health risk factors were robust to adjustment for median tract age and state. However, they were attenuated by additional adjustment for percent non-White residents in the tract, as is to be expected when controlling for a mediating variable. The adjusted R-squared for each model was also reported and the proportion of variance explained were consistent with ecological analyses of distal exposures.


Reference level: quartile 1 (low historic redlining)
A-1: Mean differences from ANOVA models of sociodemographic characteristics and COVID-19 health risk factors by quartile of national historic redlining score. First quartile is reference (I) in column one with comparison quartiles (J) in column two.